Introduction: The use of venoarterial extracorporeal membrane oxygenation (VA-ECMO) in extracorporeal cardiopulmonary resuscitation (eCPR) is an established method for selected patients (pts) in refractory cardiac arrest (CA). In the light of increasing availability, analysis of outcome-relevant predisposing pt characteristics is of growing importance. We evaluated the prognostic influence of biological gender in pts presenting with in- or out of hospital cardiac arrest (IHCA/OHCA) treated with eCPR.
Methods: We retrospectively analysed data of 330 consecutive pts treated for IHCA and OHCA using eCPR in our cardiac arrest center from the years 2016 to 2022. Primary outcome was defined as survival of the primary hospital admission with favourable neurological outcome (cerebral performance category [CPC]-score ≤2). Statistical analyses were performed using baseline comparison, survival analysis, as well as univariable and multivariable analysis.
Results: Of the 330 studied pts, 69 (21%) were of female gender. Female pts showed less prevalence of pre-existing coronary artery disease (48% vs. 75%, p<0.001) and cardiomyopathy (17% vs. 34%, p=0.01) compared to the male pts, while mean age and prevalence of other cardiovascular risk factors were balanced. Primary reason for CA differed significantly between female and male pts (female: coronary event 45%, pulmonary embolism 23%, cardiogenic shock 17%; male: coronary event 70%, primary arrhythmia 10%, cardiogenic shock 10%; p=0.001). Prevalence of witnessed collapse (97% vs. 86%; p=0.016) and performance of bystander CPR (94% vs. 85%; p=0.065) was higher in female pts. Mean time from collapse to eCPR did not differ between the two groups (77±39 min vs. 80±37 min; p=0.61). Overall, female pts showed a higher percentage of neurologically favourable survival (23% vs. 12%; p=0.027) despite a higher prevalence of procedure associated bleeding complications (33% vs. 16%, p=0.002). Multivariable analysis identified a shorter total CPR duration (p=0.001) and performance of bystander CPR (p=0.03) to be associated with superior neurological outcome. Bivariable analysis revealed relevant interactions between gender and body mass index (BMI). Male pts showed an almost linear increase of risk for an adverse outcome with increasing BMI, while female pts with very high and very low BMI values were equally at risk, with a relevant risk reduction in the range of 25 to 30 kg/m2 (figure 1).
Conclusion: In our study, female gender was was associated with significantly higher probability of favourable neurological outcome, despite higher rates of bleeding complications. These findings might be driven by anatomical differences and should exercise increased procedural awareness.
Figure 1: Logarithmic relative hazard ratio of body mass index (kg/m2) for unfavourable neurological outcome or death stratified by gender
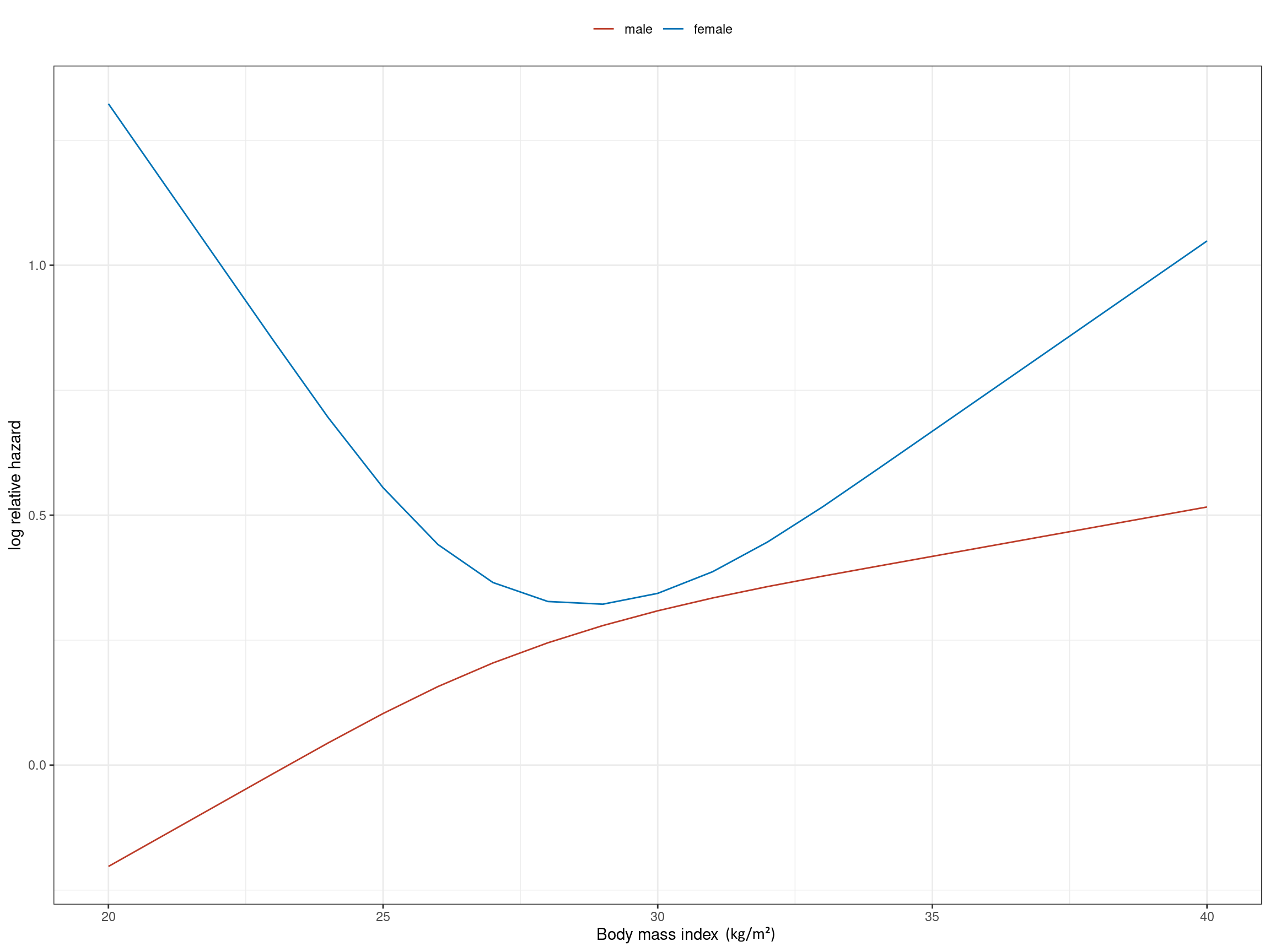
Figure 1: Logarithmic relative hazard ratio of body mass index (kg/m2) for unfavourable neurological outcome or death stratified by gender
https://dgk.org/kongress_programme/jt2023/aV1663.html