Background: Atrial tachycardias (AT) occurring after previous ablation in patients with a history of atrial fibrillation (AF) are increasingly observed in clinical practice. Catheter ablation is the treatment of choice but an optimal workflow to improve patient outcome has not been defined. The prognostic implications of baseline rhythm at the beginning of AT ablation are unknown.
Purpose: The purpose of this study was to assess procedural and clinical outcome depending on baseline rhythm during AT ablation.
Methods: A total of 380 patients (69 (61–75) years, 56.6% male) with a history of AF who underwent catheter ablation for consecutive AT after previous ablation were analyzed.
Results: At the beginning of the procedure, 140 patients (36.8%) presented in baseline sinus rhythm (SR), 208 (54.7%) with AT and 32 (8.4%) with AF. Patients in SR or with AT underwent shorter procedures (SR: 173 (132–213) minutes vs. AT: 161 (120–203) minutes vs. AF: 226 (154–249) minutes; P=0.002) with more frequent termination to SR (SR: 87.9% vs. AT: 81.3% vs. AF: 56.3%; P<0.001) than patients with AF. Periprocedural AT cycle length was longer in patients presenting in SR than in those with AT or AF (SR: 320 (265–370) ms vs. AT: 270 (240–310) ms vs. AF: 245 (193–278) ms; P<0.001). Acute procedural success did not differ between patients in SR or with AT but was higher compared to those with AF (SR: 96.4% vs. AT: 97.1% vs. AF: 87.5%; P=0.033). During a median follow-up of 290 (181–680) days, patients in baseline SR developed arrhythmia recurrences less often (SR: 36.4% vs. AT: 49.5% vs. AF: 68.8%; P=0.002) compared to patients with AT or AF.
Conclusions: Baseline rhythm at the beginning of AT ablation predicts procedural and clinical outcome. Whereas acute procedural success does not differ between patients in SR or with AT, patients presenting in SR have a more favorable mid-term success rate. Restoration of SR prior to ablation might improve long-term outcome by reducing the risk for recurrent arrhythmia.
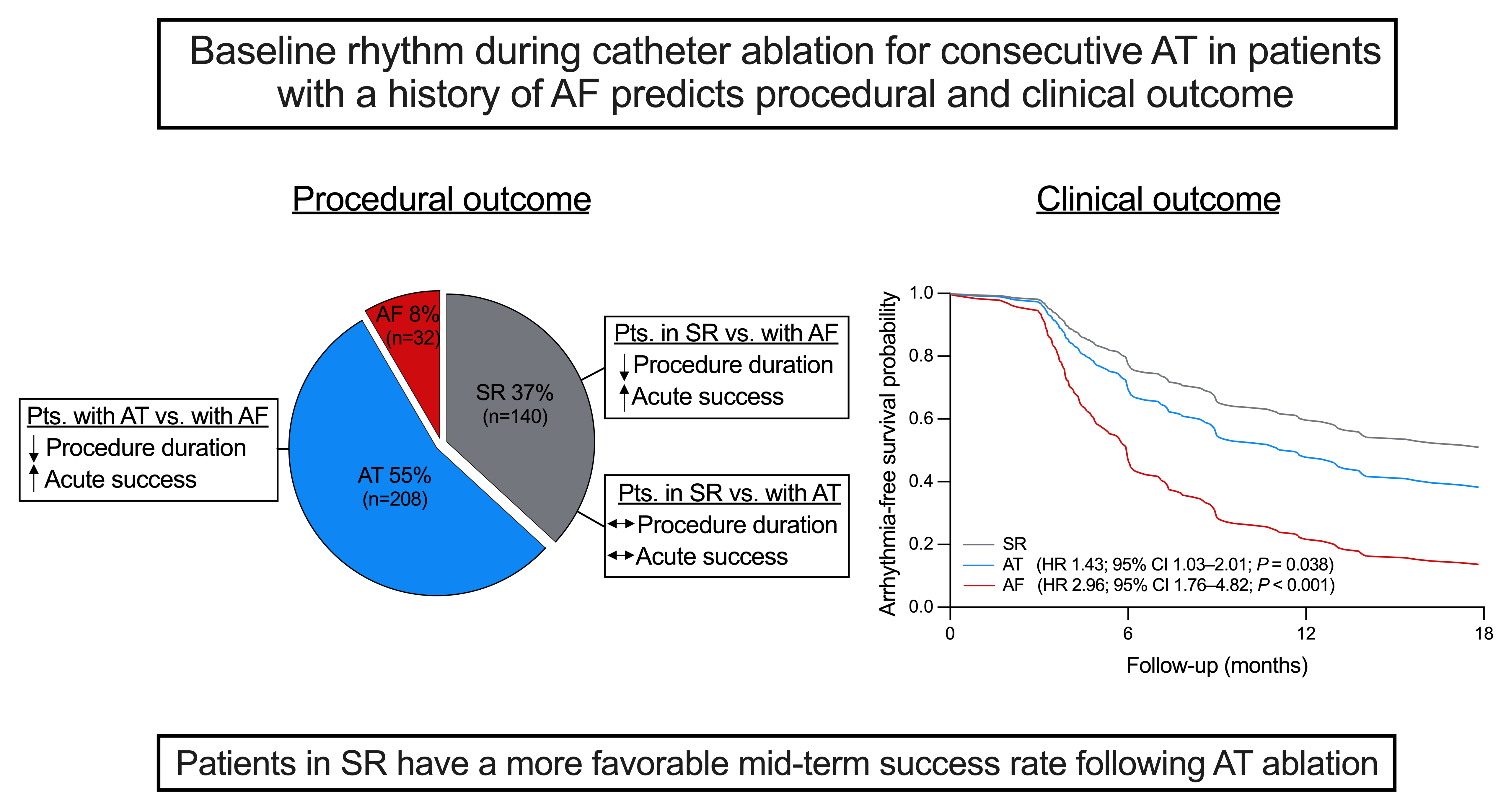
Figure: Baseline rhythm during AT ablation predicts procedural and clinical outcome.
Acute procedural success does not differ between patients in SR or with AT, but patients presenting in SR have a more favorable mid-term success rate experiencing less arrhythmia recurrences. AF, atrial fibrillation; AT, atrial tachycardia; CI, confidence interval; HR, hazard ratio; pts, patients; SR, sinus rhythm.
https://dgk.org/kongress_programme/jt2023/aP490.html