Introduction
Ischemic heart disease is a common cause of heart failure and pathological changes are increasingly assessed using cardiac MRI with late gadolinium enhancement (LGE). No-reflow zones (representing microvascular obstruction) have been associated with adverse ventricular remodelling and bad clinical outcome. Ultra-high field strength (≥7T) CMR has the potential to improve the visualization of scar heterogeneity due to higher resolution.
In a large animal study, we investigated different stages of myocardial infarction (MI). We aimed to visualize scar heterogeneity using high-resolution LGE and assess the performance of established manual and semi-automatic methods of scar size quantification and their applicability to mapping of no-reflow zones on 7T LGE images of porcine hearts.
Methods
After study approval by local authorities (Government of Lower Franconia), myocardial infarction was induced by 90 min balloon catheter occlusion of the LAD in 7 female German Landrace pigs. All pigs received a baseline MRI before, and 3 scans after the intervention (3-4, 10-14 and ~60 days after MI) and were euthanised at MRI4. LGE images (magnitude [MAG] and phase-sensitive inversion recovery [PSIR]) images were acquired on a 7T MAGNETOM™ Terra system (Siemens, Erlangen) with in vivo resolution: 0.7x0.7 mm2 and ex vivo resolution: 0.4x0.4 mm2). Infarct size was calculated using manual planimetry and semi-automatic methods (full width half maximum (FWHM) technique and n-SD technique for 3, 5 and 7 standard deviations). Manual inclusion of no-reflow zones was done in one representative scan.
Results
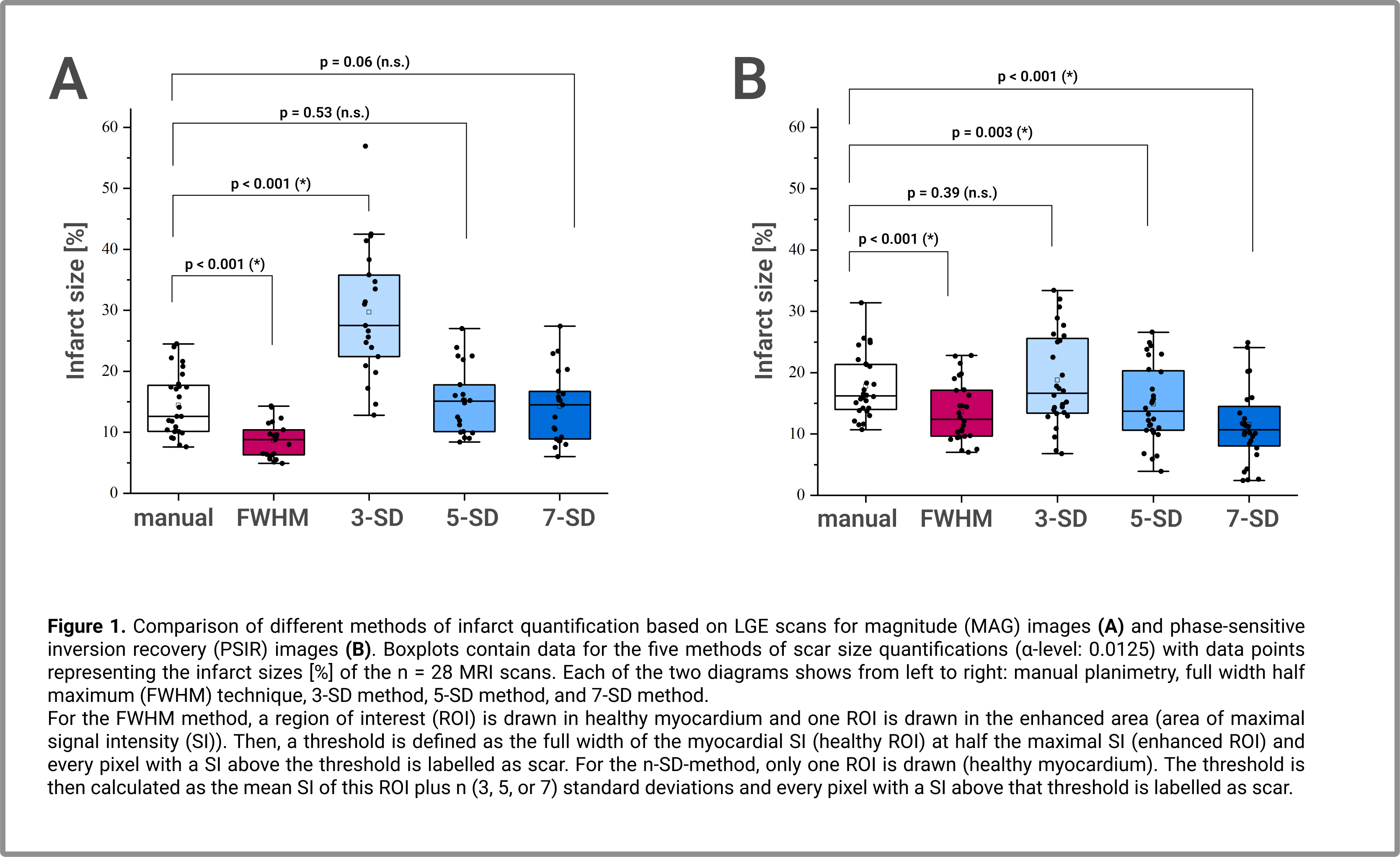
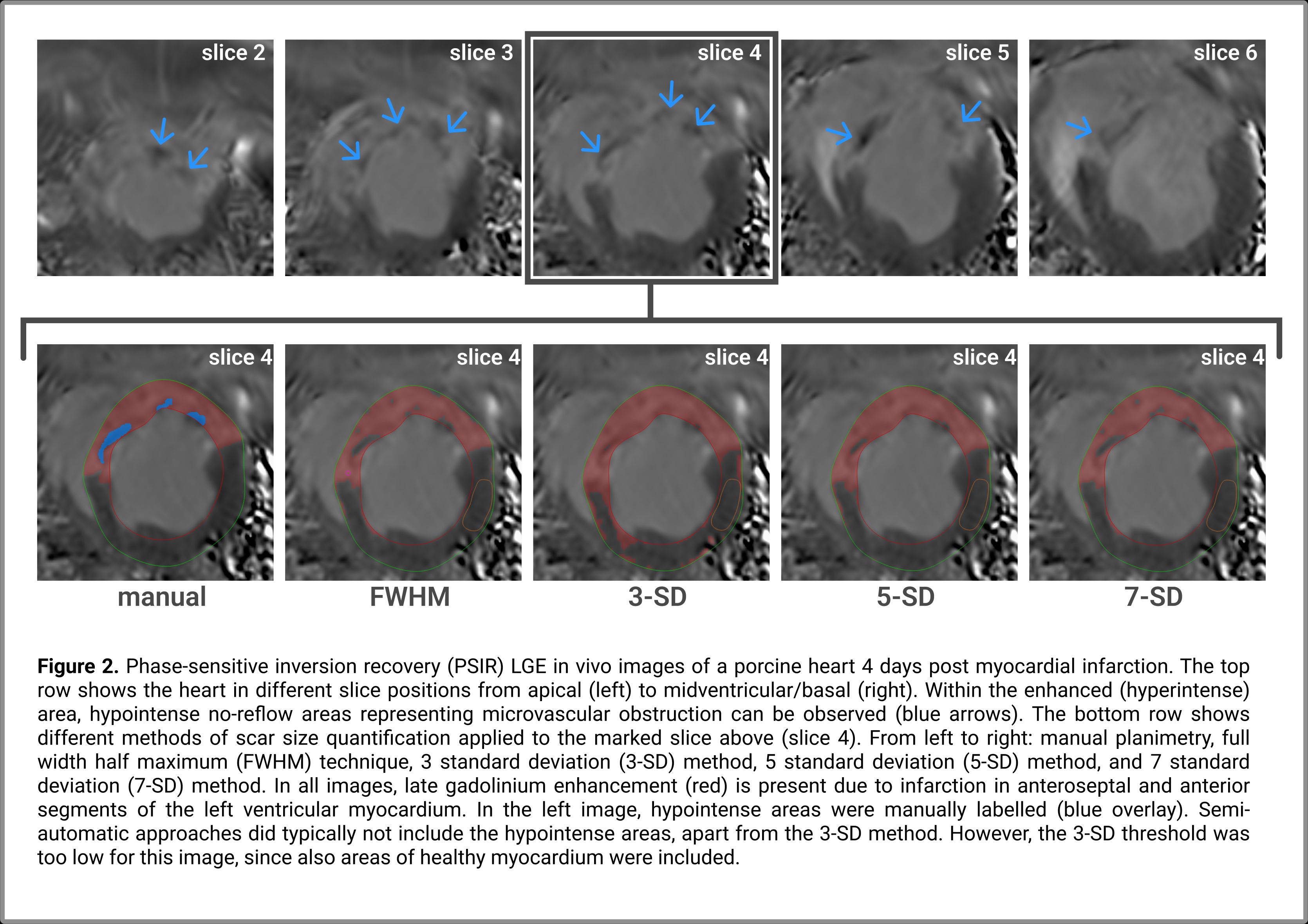
Intraclass correlation coefficients (ICCs) for intra-observer analysis were >0.9 for all methods. Semi-automatic methods for scar size quantification showed varying agreement with manual planimetry (Fig. 1). For MAG images, 5-SD and 7-SD provided visually good scar estimation and were not significantly different from manual analysis. For PSIR images, FWHM, 3-SD and 5-SD showed acceptable correlation with manual analysis (ICCs 0.70-0.81). No-reflow zones were found in some scans (Fig. 2). Labelling of hypointense no-reflow zones depended on the signal intensity of the area and the threshold of the respective semi-automatic method. In a representative case, correlation with manual analysis improved (FWHM method on PSIR images) when those areas were added manually (scar size manual: 25.3%, FWHM 21.5%, FWHMedited 23.9%). In vivo - ex vivo scar size comparison found excellent correlation for PSIR (ICC 0.94) and a moderate correlation for MAG images (ICC 0.55).
Discussion
Intra-observer agreement was excellent throughout the study. Several semi-automatic approaches correlated well with manual planimetry (ICCs: 0.70-0.92). The underestimation of scar size in vivo versus ex vivo using MAG images may be due to low blood-scar contrast in some scans, making the endocardium difficult to delineate. In addition, the small number of comparisons (n=7 for MRI4) limits statistical power.
We demonstrate that reproducible scar size quantification is possible in 7T large animal studies using several dedicated methods. Diagnostically relevant no-reflow zones can be visualized at 7T. However, for standard semi-automatic segmentation approaches, those should be added manually. Scar heterogeneity should thus be considered in future developments regarding automatic LGE segmentation.
Acknowledgements
BMBF grant: 01E1O1504
Parts of this work will be used in the thesis of AK
https://dgk.org/kongress_programme/jt2023/aP1696.html