Purpose:
Novel photon-counting detector-CT angiography using ultra-high resolution mode (UHR-
CCTA) has been shown to be feasible for coronary imaging. However, correlation with
invasive coronary angiography has not yet been thoroughly investigated. Here, we compare
UHR-CCTA with invasive quantitative coronary angiography (QCA) as the gold standard.
Methods:
Retrospective analysis including all consecutive patients who had undergone UHR-
CCTA for the assessment of coronary artery disease with subsequent clinically indicated
coronary angiography within 30 days from CCTA at the University Medical Center Mainz
since 07/2022. Exclusion criteria were a chronic total coronary occlusion and prior coronary
intervention. In addition to a standard reconstruction with 0.6 mm slice thickness, datasets
with 0.4 mm slice thickness as well as a UHR reconstruction with 0.2 mm slice thickness were
obtained. Degree of stenosis as assessed by invasive QCA (CAAS, Pie Medical Imaging) and
quantitative CCTA (Syngo.via, Siemens Healthcare) were compared using univariate analysis
of variance with post-hoc testing and Bland-Altman plots.
Results:
A total of 23 patients were included (mean age 71.0 ± 8.6 years; 74% males; mean
BMI 29±7 kg/m 2 ; mean heart rate 66±7 bpm). CT identified 50 coronary stenoses with a
mean degree of 62.9±17.6% in the 0.6 mm datasets which declined with significantly
decreasing slice thickness (0.4 mm: 58.7±18.5%; UHR 0.2 mm: 51.9±19.9%; both p≤0.001).
When comparing with invasive measurement, the 0.6 mm reconstruction significantly
overestimated degree of stenosis with QCA (49.4±18.2%, p=0.002), but not the 0.4 and UHR
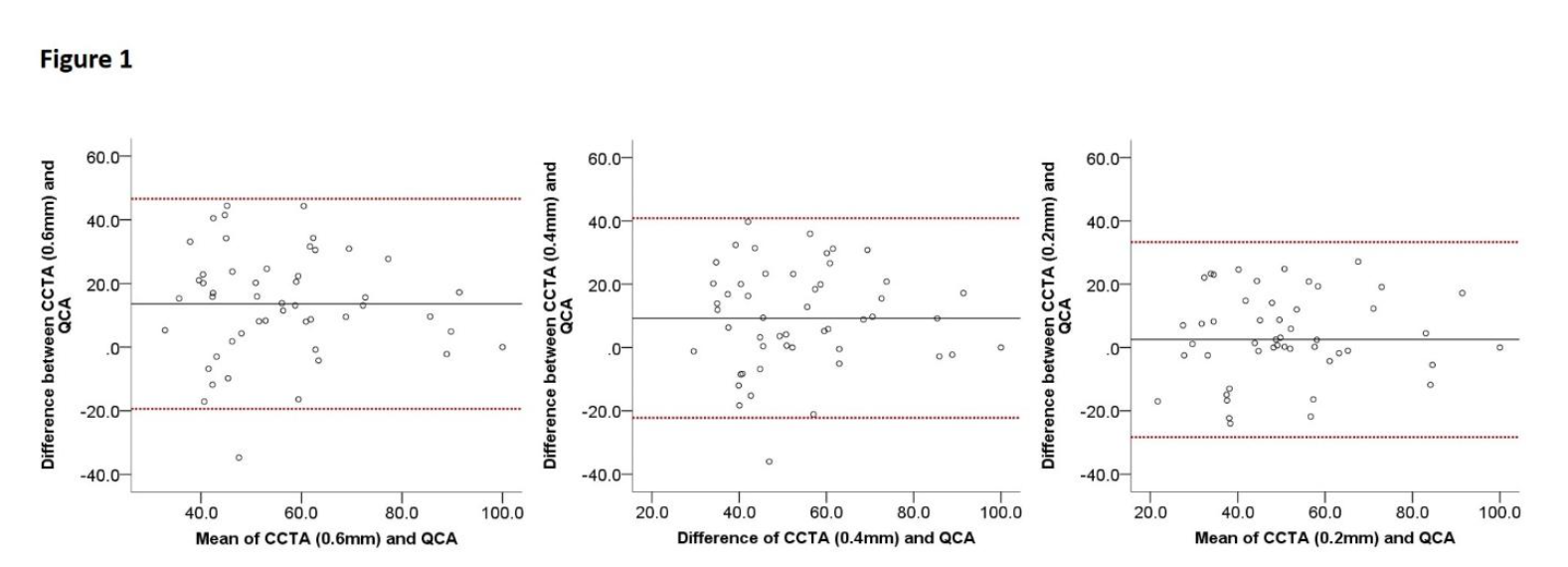
0.2 mm reconstructions (p=0.82 and p=1.0). Bland Altman analysis revealed a significant bias
between 0.6 mm (mean bias 13.6, limits of agreement 3.6.6 to 23.5, Figure 1) and 0.4 mm
(9.3, -0.6 to 19.2) reconstructions with QCA, respectively. UHR 0.2 mm reconstruction did
not show a clinically significant bias with the gold standard (2.5, -7.4 to 12.4).
Conclusions:
In this early clinical photon-counting detector-CT study, UHR-CCTA showed an
improved correlation with invasive QCA compared to a standard CT reconstruction. Larger
trials are necessary to investigate the potential for reducing unnecessary referral for follow-
up invasive imaging.
https://dgk.org/kongress_programme/ht2023/aV87.html